Categories
Change Password!
Reset Password!


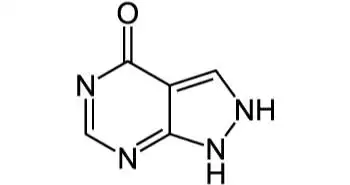
Allopurinol is a structural analog of the natural purine base, hypoxanthine.
Allopurinol is a structural analog of the natural purine base, hypoxanthine. It is considered to be one of the most effective drugs used to decrease urate levels and is approved by the FDA for management of gout, calcium oxalate stones and cancer therapy-induced hyperuricemia. It is also recommended as a part of urate-lowering therapies in chronic persistent gouty arthritis, tophaceous gout, uric acid urolithiasis.
Pharmacological
class: Xanthine Oxidase Inhibitors
Allopurinol acts by
inhibiting xanthine oxidase, the enzyme responsible for
the conversion of hypoxanthine to xanthine and of xanthine to uric acid. It
leads to reduced production of uric acid, resulting in a decrease of urate
levels and relief of symptoms associated with gout such as painful tophi, joint
pain, inflammation, redness, decreased range of motion, and swelling.
Usual Adult Dose for Gout
Usual Adult Dose for prevention of uric acid nephropathy during the therapy of neoplastic disease
Usual Adult Dose for management of recurrent calcium oxalate stones
Absorption:
Approximately 90% of the drug is absorbed from the
gastrointestinal tract. Peak plasma levels normally occur at 1.5 hours
post-dose for allopurinol. Maximum plasma levels observed after one oral dose
of 300 mg of allopurinol are 3 mcg/mL.
Volume
of distribution (Vd): Allopurinol is a substrate for enzyme xanthine
oxidase, present in the cytoplasm of endothelial cells of capillaries and
highest activity in the liver and intestinal lining. Human studies for tissue
concentrations of allopurinol have not been reported, but in animal studies, it
has been found to reach highest levels in blood, liver, intestine and heart,
and lowest in the brain and lung tissues.
Protein
binding: Allopurinol is negligibly bound to plasma
proteins
Metabolism: Allopurinol is rapidly metabolized to the corresponding xanthine analogue, oxypurinol (alloxanthine), an inhibitor of xanthine oxidase enzyme. It is converted to their respective ribonucleotides by the purine salvage pathway. The effect of these ribonucleotides related to the hypouricemic action of allopurinol in humans is not fully elucidated.
Route of elimination: Approximately 80% of orally ingested allopurinol is excreted in the urine, and 20% of ingested allopurinol is excreted in the faeces.
Half-life: The plasma half-life of allopurinol is 1-2 hrs due to rapid renal clearance
Clearance:
Allopurinol and its metabolites are mainly
eliminated by the kidney; therefore, the dose should be reduced as the drug can
accumulate in patients with renal failure. A daily dosage of 200 mg allopurinol
is suitable in case of creatinine clearance of 10 to 20 mL/min whereas the
daily dosage should not be higher than 100 mg in case of creatinine clearance
less than 10 mL/min.
Allopurinol is widely prescribed as first line
urate lowering therapy in gout patients. Serum uric acid (sUA) levels are frequently not achieved due
to percieved intolerability of doses above 300 mg. Studies related to the
efficacy and safety of allopurinol at doses above 300 mg/day are limited.
Evidences from a large open label, 6 month study (LASSO) indicated the
sUA-lowering efficacy, gout flare
frequency and safety of dose-titrated allopurinol by clinical and laboratory
examinations at monthly visits. A total
of 1735 patients were enrolled and categorised in three categories: Category
one (< 300 mg), Category two (300 mg) and Category three (> 300 mg). The
results showed that allopurinol was well tolerated with low rates of treatment
related adverse events (TEAEs) and discontinuation-related TEAEs. The most
common TEAEs were diarrhea, upper respiratory tract infection, and arthralgia.
Nephrolithiasis was also reported in 7 patients in the 300mg allopurinol
category. The incidence of skin rash and allopurinol hypersensitivity syndrome
(AHS) were low. Serious adverse events (SAEs) were observed in 51 patients. The
various SAEs includes pneumonia, acute myocardial infarcation, cellulitis,
diverticulitis, prostate cancer, gout, acute coronary syndrome, atrial fibrillation,
atrial flutter, supraventricular tachycardia, and small intestinal
obstruction. Two patients in the 300-mg
category and one patient in the < 300-mg category had an SAE with outcome of
death, categorized respectively as sudden death, pulmonary embolism, and death
due to natural causes.
Other common TEAEs associated with allopurinol
withdrawal or study discontinuation were rash, diarrhea, increase in alanine
aminotransferase and gamma glutamyl transferase. The overall incidence of MACE
(CV death, nonfatal MI, and nonfatal stroke) was 0.58%, with an incidence rate
of 1.42/100 patient-years (95% CI 0.68–2.61). The incidence of non-MACE CV end points was 0.75%. In conclusion, there were minor differences
the incidence of TEAEs possibly related to allopurinol between the dosing
categories (< 300 mg, 300 mg, and > 300 mg daily). The allopurinal doses
were well tolerated without new safety signals emerging over 6 months.
Gout: A cohort study was conducted by Li Wei et al. to study the impact of allopurinol on the urate levels and cardiovascular outcomes associated with gout. A total of 7135 patients aged ≥60 years with urate measurements between year 2000 and 2002 followed up until 2007 were included. Six thousand and forty-two patients refused to take urate-lowering therapy (ULT), and 45.9% of participants had urate concentrations ≤6 mg dl−1. Among 1035 participants administered with allopurinol, 44.7% reached target urate levels. No significant increase in risk of cardiovascular events was observed for allopurinol users as compared to non-ULT users and the non-ULT group with urate >6 mg dl−1. Cardiovascular events rates were 74.0 per 1000 person-years for the 100 mg group, 69.7 for the 200 mg group and 47.6 for the ≥300 mg group within allopurinol use cohort. High dose users had significant reductions in the risk of cardiovascular events and mortality as compared to patients administered with low dose allopurinol. Less than 50% of patients receiving allopurinol reached urate concentrations. In conclusion, higher doses of allopurinol were associated with better control of urate and lower risks of both cardiovascular events and mortality.
Calcium oxalate
stones: A double blind study was conducted by
Ettinger B et al. to examine the efficacy of allopurinol in the
prevention of recurrent calcium oxalate calculi of the kidney. A total of sixty
patients with hyperuricosuria and normocalciuria with a previous history of
calculi were randomly categorised to receive either allopurinol (100 mg three
times daily) or a placebo. The findings of study indicated a significant
decrease in calculi in allopurinol group (81.2%) as compared to placebo (63.4%).
The mean rate of calculous events was 0.26/patient/year in the placebo group
and 0.12 in the allopurinol group. The comparison of treatment groups by
actuarial analysis showed a significantly longer time before recurrence of
calculi in allopurinol group. The study concludes that allopurinol is effective in the prevention
of calcium oxalate stones in patients with hyperuricosuria.










Comments (0)