Categories
Change Password!
Reset Password!


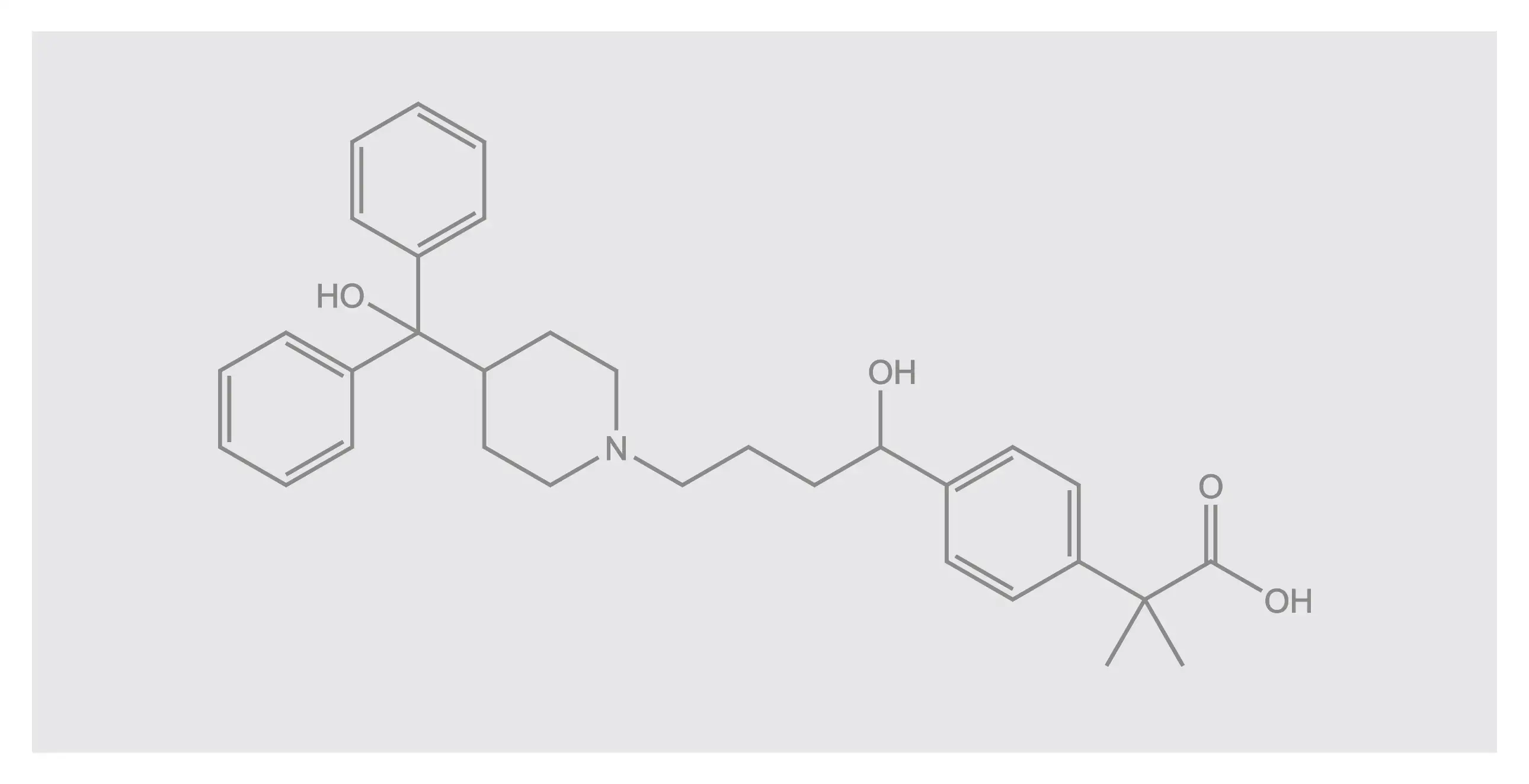
Fexofenadine, a selective H1-antagonist and second-generation antihistamine, is FDA-approved to treat symptomatic seasonal allergic rhinitis and chronic idiopathic urticaria.
Fexofenadine, a selective H1-antagonist and second-generation antihistamine, is FDA-approved to treat symptomatic seasonal allergic rhinitis and chronic idiopathic urticaria. It has approval for use in both adults and children. It does not cross the blood-brain barrier and therefore does not elicit drowsiness when compared to H1 blockers. Furthermore, it has less affinity for alpha-adrenergic and cholinergic receptors and thus does not exhibit anticholinergic adverse effects in comparison with other antihistamine agents. [1]
Pharmacological Class: Antihistamines [2]
Fexofenadine (second-generation H1 receptor blocker) is indicated for the treatment of:
For mediation of allergic and hypersensitivity reactions, the H1 histamine receptor is accountable. Exposure to an allergen triggers degranulation of basophils and mast cells. This results in liberation of histamine and other mediators of inflammation. Histamine binds to H1 receptors and results in its activation. This, in turn, liberates pro-inflammatory cytokines (like interleukins) from mast cells and basophils. These downstream impact of histamine binding are accountable for a vast range of symptoms of allergy, like watery eyes, rhinorrhea, and pruritus.
Fexofenadine is deemed as an “inverse agonist” of H1 receptor. It has a selective and potent affinity for H1 receptors. It binds to and stabilizes inactive form of receptor. This, in turn, prevents its activation and subsequent downstream impact. [4] Fexofenadine selectively antagonizes H1 receptors on surface of cells. It is non-sedating and affects the inflammatory mediators. It can also suppress other mechanisms like mast cell, basophilic histamine, and inflammatory cell release. [1]
(I) Adult Dosing
(II) Pediatrics Dosing (differs based on age and indication)
(III) Special Population
Dosing for pediatric patients with renal impairment varies by age as follows:
(a) Children older than twelve years: 60 mg PO daily
(b) Children two-twelve years old: 30 mg PO daily
(c) Children six months to two years old: 15 mg PO daily [1]
Absorption
After the oral administration of fexofenadine, it is rapidly absorbed with a bioavailability of about 33%. Post-administration Tmax is about 1 to 3 hours. The steady-state area under curve [AUCss (0-12h)] and Cmax after receiving 60 mg dosing twice daily are 1367 ng/mL.h and 299 ng/mL.
The AUC of fexofenadine is lowered by >20% when concomitantly administered with fruit juices due to their suppression of OATP transporters. It is recommended to take fexofenadine with water only. Likewise, fexofenadine coadministration with high-fat food seems to lower the Cmax and AUC by >20%.
Volume of distribution
Fexofenadine's volume of distribution is around 5.4-5.8 L/kg
Protein binding
There is 60-70% binding of fexofenadine with plasma proteins, majorly with albumin and α1-acid glycoprotein. In people with hepatic and renal impairment, the degree of protein binding is decreased to 56-75% and 56-68%
Metabolism
Fexofenadine is slightly metabolized, with only 5% of consumed dosage undergoing liver metabolism. MDL 4829 and methyl ester of fexofenadine are the only identified metabolites
Route of elimination
Elimination of ingested dose is via faeces (80%), and 11% through urine. Renal and biliary are the major pathways for the elimination of fexofenadine
Half-life
The terminal elimination half-life of fexofenadine is found to be about 11-15 hours
Clearance
The renal clearance of fexofenadine is approximately 4.32 L/h and the oral clearance is around 50.6 L/h[4]
The most commonly reported adverse effects are:
(a) Allergic rhinitis
In a systematic review and meta-analysis carried out by Huang CZ et al., fexofenadine exhibited a positive antihistamine effect with a favorable safety profile. Overall, 51 trials and 14,551 participants were included to compare safety and antihistamine effects of fexofenadine with either placebo or other antihistamine agents for healthy subjects and people with allergies.[6]
According to a phase 3, randomized, double-blind trial conducted by Anne K. Ellis et al. in 251 people with seasonal allergic rhinitis, fexofenadine HCl (180 mg) was efficient in ameliorating pollen-induced, air pollution-exacerbated symptoms of allergic rhinitis. [7]
A review demonstrated that compared to placebo, fexofenadine can effectively relieve nasal congestion linked with allergic rhinitis. [8] A study by Okubo K et al. reported that administration of fexofenadine HCl (60 mg twice a day) can elicit significant improvement in overall quality of life and work productivity in people with seasonal allergic rhinitis. [9]
(b) Urticaria
A quasi-experimental study aimed to explore efficacy of fexofenadine in 100 patients (aged 18 years and above) with chronic idiopathic urticaria. Participants received 120 mg of fexofenadine twice daily for four weeks. Following 4 weeks of therapy, 42% reported complete disappearance of symptoms, 24% exhibited marked improvement, 26% had moderate improvement, and 8.0% illustrated slight improvement. Fexofenadine was highly efficient in alleviating chronic idiopathic urticaria.[10]
In a network meta-analysis, fexofenadine demonstrated superior therapeutic efficacy (in terms of total symptom score [TSS] changes from baseline) when compared to placebo for treatment of people diagnosed with chronic spontaneous urticaria. [11] A narrative review suggested that second-generation antihistamines like fexofenadine HCl can considerably reduce urticaria symptoms such as wheals and angioedema. [12] In a systematic literature review, high doses of fexofenadine were found to elicit a significant dose-dependent response and controlled urticaria in most of the patients. [13]










Comments (0)