Categories
Change Password!
Reset Password!


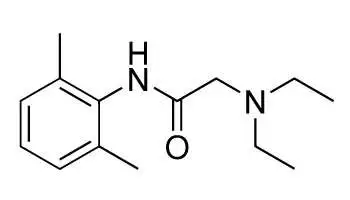
Lidocaine is a synthetic aminoethylamide with local anesthetic properties.
Lidocaine is a synthetic aminoethylamide with local anesthetic properties. Lidocaine is used on different parts of the body to cause numbness or loss of feeling for patients having certain medical procedures. It is also used to relieve pain and itching caused by conditions such as sunburn or other minor burns, insect bites or stings, poison ivy, poison oak, poison sumac, minor cuts, or scratches.
Pharmacological class: Local Anesthetic
Lidocaine stabilizes the neuronal membrane by inhibiting the ionic fluxes required for the initiation and conduction of impulses thereby effecting local anesthetic action. Lidocaine alters signal conduction in neurons by blocking the fast voltage gated sodium (Na+) channels in the neuronal cell membrane that are responsible for signal propagation. With sufficient blockage the membrane of the postsynaptic neuron will not depolarize and will thus fail to transmit an action potential. This creates the anesthetic effect by not merely preventing pain signals from propagating to the brain but by aborting their birth in the first place.
Usual Adult Dose for Anesthesia: Dose varies with procedure, degree of anesthesia needed, vascularity of tissue, duration of anesthesia required, and physical condition of patient.
Maximum dose: 4.5 mg/kg/dose; do not repeat within 2 hours.
Bioavailability of lidocaine is variable and mainly dependent on adrenaline supplement and local blood flow. The peak plasma level is 15 to 30 minutes and plasma half-life accounts for 30-90 minutes. The elimination is predominantly hepatic.
Common (affecting between 1 in 10 to 1 in 100):
Uncommon (affecting 1 in 100 to 1 in 1000):
Very rare (affecting less than 1 in 10,000):
In 8 trials, total 161 patients received intravenous lidocaine, with 159 controls. Intravenous lidocaine administration decreased the duration of ileus (weighted mean difference (WMD) - 8.36 h), length of hospital stay (WMD - 0.84 days), postoperative pain intensity at 24 h after operation on a 0-100-mm visual analogue scale (WMD - 5.93 mm), and the incidence of nausea and vomiting (odds ratio 0.39). Continuous intravenous administration of lidocaine during and after abdominal surgery improves patient rehabilitation and shortens hospital stay1
One hundred sixteen adults having complex spine surgery were randomly assigned to perioperative IV lidocaine (2mg·kg·h) or placebo during surgery and in the post anesthesia care unit. Pain was evaluated with a verbal response scale. Quality of life at 1 and 3 months was assessed using the Acute Short-form (SF) 12 health survey. The authors initially evaluated multivariable bidirectional noninferiority on both outcomes; superiority on either outcome was then evaluated only if noninferiority was established. Lidocaine was significantly superior to placebo on mean verbal response scale pain scores and significantly non-inferior on mean morphine equivalent dosage. Postoperative nausea and vomiting and the duration of hospitalization did not differ significantly. Patients given lidocaine had slightly fewer 30-day complications than patients given placebo. Patients given lidocaine had significantly greater SF-12 physical composite scores than placebo at 1 and 3 months, postoperatively.2










Comments (0)