Categories
Change Password!
Reset Password!


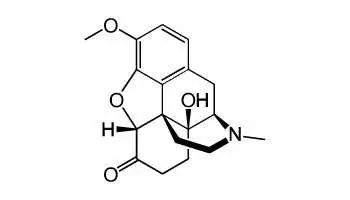
Oxycodone is a phenantherne derivative with opioid analgesic activity similar to morphine but adverse effects are milder than those of morphine. Oxycodone is used to control moderate to severe pain, including postoperative, post extractional, and postpartum pain and other opiates such as morphine and codeine act as agonists at opiate receptors within the central nervous system (CNS).
Oxycodone is a phenantherne derivative with opioid analgesic activity similar to morphine but adverse effects are milder than those of morphine. Oxycodone is used to control moderate to severe pain, including postoperative, post extractional, and postpartum pain and other opiates such as morphine and codeine act as agonists at opiate receptors within the central nervous system (CNS).
Pharmacological Class: Opioid analgesic
Oxycodone is a pure opioid agonist whose principal therapeutic action is analgesia. The mechanism of action of oxycodone involves: binding to mu-type opioid receptors, inhibition of adenylyl-cyclase and hyperpolarisation of neurons, and decreased excitability. However, binding to the opiate receptors in CNS causes an inhibition of ascending pain pathways, alteration of the perception and response to pain and produces generalized CNS depression.
Common (affecting between 1 in 10 to 1 in 100)
Uncommon (affecting 1 in 100 to 1 in 1000)
Very rare (affecting less than 1 in 10,000)










Comments (0)