Categories
Change Password!
Reset Password!


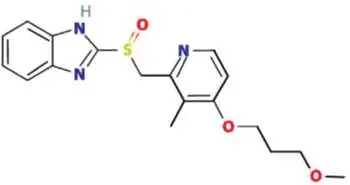
Rabeprazole
is a proton-pump inhibitor (PPI) that lowers the amount of acid produced in the
stomach.
Rabeprazole is a proton-pump inhibitor (PPI) that lowers the amount of acid produced in the stomach. This substituted benzimidazole PPI belongs to the class of antisecretory compounds. [1]
Pharmacological Class: Proton Pump Inhibitor (PPI)
It is indicated[2];
(a) In pediatric patients 1
to 11 years of age
(b) In adults for:
(b) In adolescent patients 12
years of age and older for:
Rabeprazole inhibits the
secretion of gastric acid by suppressing the gastric H+ , K+ ATPase
(hydrogen-potassium adenosine triphosphatase) at the secretory surface of the
gastric parietal cell. However, this gastric proton-pump inhibitor does not
demonstrate anticholinergic or histamine H2-receptor antagonist properties. It
hinders the final step of secretion of gastric acid. In the parietal cells,
rabeprazole is protonated, accumulates, and is potentially transformed to an
active sulfenamide. [3]
|
Healing of erosive or ulcerative GERD |
20 mg once daily four to eight weeks |
|
Maintenance of healing of erosive or ulcerative GERD |
20 mg once daily |
|
Treatment of symptomatic GERD in adults |
20 mg once daily for four weeks |
|
Healing of duodenal ulcers |
20 mg once daily after the morning meal for up to four
weeks |
|
H. pylori elimination to lower risk of duodenal ulcer
recurrence
Three drug regimen: Rabeprazole 20 mg Amoxicillin 1000 mg Clarithromycin 500 mg |
All three medications should be taken twice daily with
evening and morning meals for seven days. |
|
Treating pathological hypersecretory conditions, including
Zollinger-Ellison Syndrome |
Initial dose 60 mg once daily then adjust to requirements
of patients |
|
Treating symptomatic GERD in adolescents 12 years of age
and older |
20 mg once daily for up to eight weeks |
|
Treating GERD in 1- to 11-year-olds |
Less than 15 kg: 5 mg once daily (with the choice to rise
to 10 mg once daily) 15 kg or greater: 10 mg once daily for up to 12 weeks |
Absorption
Absolute bioavailability is about 52%.
0.34 L/kg*
96.3% bound to human plasma proteins
Rabeprazole is metabolized to the active metabolite of rabeprazole
After a single 20 mg oral dose of 14C-labeled rabeprazole, about 90% of rabeprazole was excreted via urine, primarily as thioether carboxylic acid; its glucuronide, and mercapturic acid metabolites. The remainder dose was recovered in stools.
1-2 hours (in plasma)
Not Available
History of hypersensitivity
to rabeprazole[2]
Rabeprazole has comparable H. pylori elimination rates as omeprazole [4]
A study demonstrated that in acid-peptic disorder patients having H. pylori infection, rabeprazole has comparable H. pylori elimination rates in comparison with omeprazole when co-administered with the antibiotics like clarithromycin and amoxicillin for about two weeks.
A study was carried to investigate the efficacy of rabeprazole (20 mg) vs. omeprazole (40 mg) in the triple therapy regimen. Overall, 100 H. pylori-infected patients who gave their consent for trial participation were incorporated. In total, 50 subjects were given omeprazole-based triple treatment and the other 50 subjects were given rabeprazole-based triple treatment. Following two weeks of triple therapy and four weeks of proton pump inhibitor therapy, H. pylori antigen was tested in stools.
A substantial correlation was noted between nausea,
epigastric pain, and water brash with a p-value, 0.001. Similarly, the p-value
was < 0.05 between bile reflux, hiatus hernia, and reflux and the p-value
was < 0.001 among hiatus hernia and reflux. In the follow-up assessment,
after triple therapy, H. pylori antigen tests were found to be negative in
about 94% of the trial population, who were administered rabeprazole which
displayed similarity to omeprazole-recipients (92%). Both rabeprazole and
omeprazole have comparable H. pylori elimination rates when
co-administered with antibiotics like clarithromycin and amoxicillin for two
weeks.
Triple therapy containing
rabeprazole is effective to treat H. pylori infection [5]
A study illustrated that a 14-day course has superior efficacy in comparison with the 10-day course of triple therapy (rabeprazole, amoxicillin, and clarithromycin) as a first-line for eliminating H. pylori infection. A double-blinded, prospective, randomized clinical trial was carried to investigate the efficacy of a 10-day vs a 14-day course of triple therapy to treat H. pylori infection.
Overall, 75 participants were randomly allocated to receive triple therapy as 20 mg rabeprazole, 1000 mg amoxicillin, and 500 mg clarithromycin twice daily for 14 days (n=38) or 10 days plus four days placebo (n=37). Elimination was determined with a urea breath test at least four weeks after completion of the therapy. The elimination rate for the 10-day cohort and the 14-day cohort in the intention-to-treat analysis and the per-protocol analysis is shown in the following table:
|
Elimination rate |
10-day cohort |
14-day group |
|
Intention-to-treat analysis |
67.6% |
86.8% |
|
Per-protocol analysis |
73.5% |
91.9% |
Table 1: Comparison of H.
pylori elimination rate
Adverse events were not
considerably different between the two cohorts. Thus,
the 14-day course is superior compared to a 10-day course triple therapy to
eliminate H. pylori.
*Swan Hoyumpa Merritt. Review article: the pharmacokinetics
of rabeprazole in health and disease. Alimentary Pharmacology and Therapeutics.
Volume 13, Issues 3 August 1999 Pages 11-17.












Comments (0)