Categories
Change Password!
Reset Password!


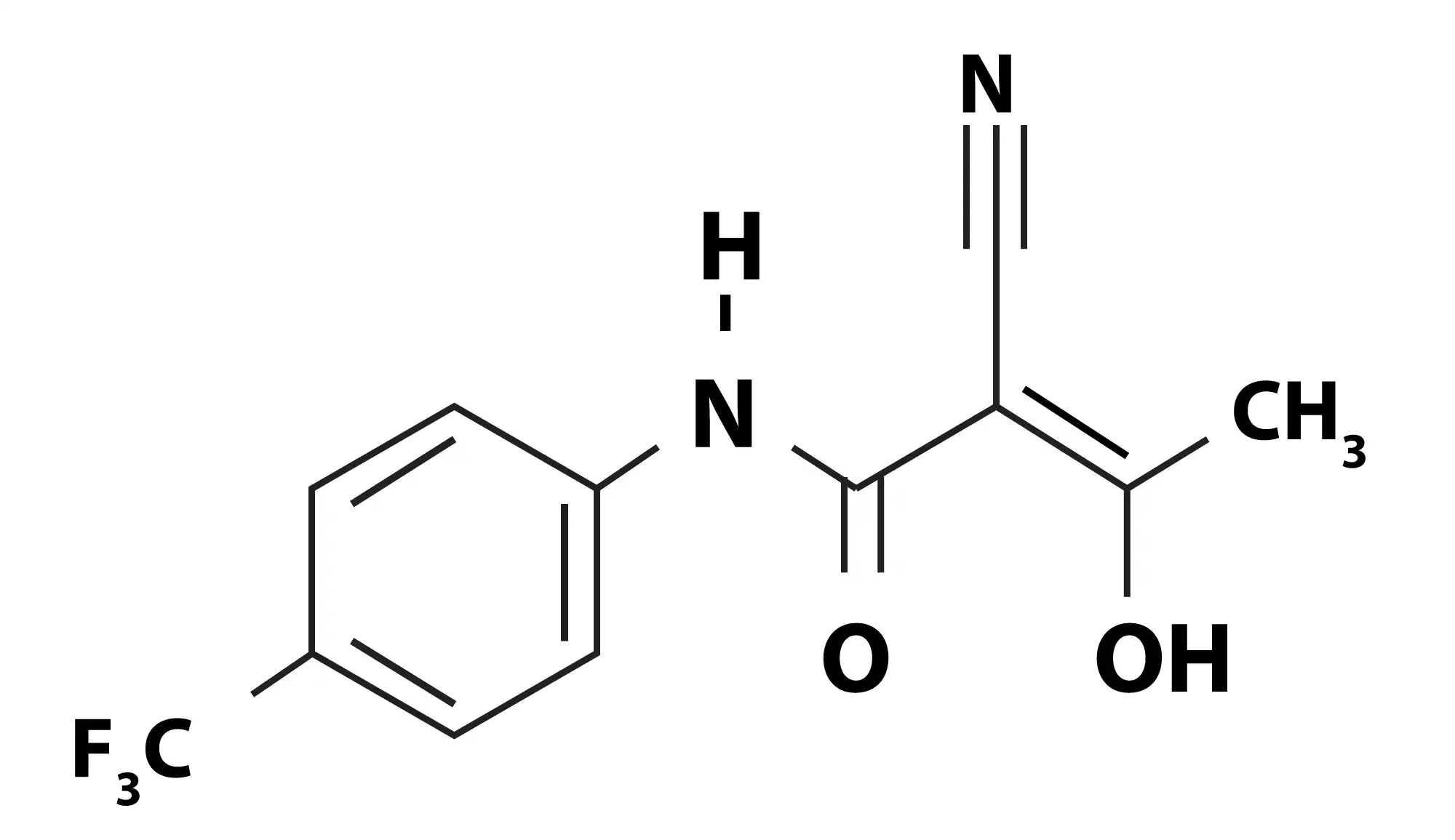
Teriflunomide, a pyrimidine synthesis inhibitor with immunomodulatory and anti-inflammatory characteristics, is utilized to cure people suffering from multiple sclerosis.[1] On 12 September 2012, teriflunomide was approved by FDA. [2]
Teriflunomide, a pyrimidine synthesis inhibitor with immunomodulatory and anti-inflammatory characteristics, is utilized to cure people suffering from multiple sclerosis.[1] On 12 September 2012, teriflunomide was approved by FDA. [2]
Pharmacological Class: Immunomodulatory agents [3]
Teriflunomide is utilized for the treatment of relapsing-remitting forms of multiple sclerosis.[1]
Teriflunomide leads to inhibition of dihydroorotate dehydrogenase, a mitochondrial enzyme implicated in the synthesis of de novo pyrimidine. [4] Suppression of dihydroorotate dehydrogenase restricts the available pyrimidine pool for the proliferation of B- and T-cells. This lowers the number of activated T and B cells available to cross blood-brain barrier and enter central nervous system. Hence, during teriflunomide therapy, the immune responses are preserved. [5] This might be involved in the immunomodulatory effect of teriflunomide in multiple sclerosis. [1]
The suggested dose is 7 mg or 14 mg taken orally once daily, without or with food. [4]
Absorption
The maximum plasma concentrations are reached in approximately 1 to 4 hours, after oral teriflunomide therapy.
Volume of distribution
The volume of distribution after the single intravenous dose of teriflunomide is 11 L.
Protein binding
Teriflunomide is extensively plasma protein bound (>99%).
Metabolism
Teriflunomide majorly undergoes hydrolysis to minor metabolites. Other minor metabolic pathways include sulfate conjugation, N-acetylation and oxidation. CYP450 or flavin monoamine oxidase do not metabolize teriflunomide.
Route of elimination
It is eliminated unaltered and primarily via bile. Particularly, 22.6% is eliminated in the urine and 37.5% in the feces.
Half-life
The median half-life is 18-19 days.
Clearance
Following a single intravenous dose, teriflunomide's total body clearance is 30.5 mL/h. [1]
Teriflunomide is contraindicated in people with:
The most commonly reported side effects are:
Long-term effectiveness and safety of teriflunomide in people having relapsing multiple sclerosis
In a recent study, 14 mg teriflunomide was well-tolerated and demonstrated long-term safety and effectiveness up to 6.3 years in people with relapsing forms of multiple sclerosis. This study reported the long-term efficacy and safety outcomes of teriflunomide from the TOWER extension study. Out of 751 people in TOWER extension study, 233, 265, and 253 people were given teriflunomide 14 mg/14 mg, teriflunomide 7 mg/14 mg, and placebo/teriflunomide 14 mg respectively.
The relapse activity and disability advancement remained low and stable over time. The occurrence of side effects was comparable to the TOWER core study. No novel or unexpected side effects were witnessed. The findings supported teriflunomide's positive benefit-risk profile as a long-term immunomodulatory treatment. [6]
Pooled post hoc analysis of long-term efficacy and safety of teriflunomide in relapsing multiple sclerosis
In another post hoc analysis, data were pooled from phase II and phase III TENERE, TOWER, and TEMSO clinical trials and their extension studies. Teriflunomide's long-term efficacy and safety were assessed in subgroups of people with relapsing multiple sclerosis defined by previous treatment status. Teriflunomide 14 mg effectiveness and safety was similar in all the patients, irrespective of previous treatment history. [7]
Teriflunomide vs. placebo for relapsing multiple sclerosis management
A subgroup assessment of the Phase 3 TOWER Study was carried out to examine safety and effectiveness of two teriflunomide doses (14 mg, 7 mg) in the Chinese subpopulation (subgroup of Chinese people) with relapsing multiple sclerosis incorporated in the TOWER study. A total of 148 volunteers were randomly allocated to get either 7 mg teriflunomide (n = 51), 14 mg teriflunomide (n = 43), or placebo (n = 54).
In comparison with the placebo, 14 mg teriflunomide decreased the twelve-week confirmed disability worsening by 68.1% and also profoundly minimized the annualized relapse rates. Teriflunomide showed good efficacy, safety, and tolerability profile in the Chinese subpopulation. [8]
Meta-analysis on teriflunomide's efficacy and safety in relapsing multiple sclerosis
In a meta-analysis of randomized controlled trials, teriflunomide substantially minimized the frequency of annualized relapse rates and disability progression with a comparable safety and tolerability profile when compared to placebo. [9]
1. Teriflunomide. Drug Bank. Accession Number DB08880. Available online from: https://go.drugbank.com/drugs/DB08880 [Last accessed on: 5 March 2022]
2. Cada DJ, Demaris K, Levien TL, Baker DE. Teriflunomide. Hospital Pharmacy. 2013 Mar;48(3):231-40.
3. Teriflunomide. Available online from: https://medlineplus.gov/druginfo/meds/a613010.html#:~:text=Teriflunomide%20is%20in%20a%20class,that%20may%20cause%20nerve%20damage. [Last accessed on: 5 March 2022]
4. Teriflunomide. FDA LABEL. Available online from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2012/202992s000lbl.pdf
[Last accessed on: 5 March 2022]
5. Teriflunomide in multiple sclerosis: an update. Available online from: https://www.futuremedicine.com/doi/10.2217/nmt-2016-0029 [Last accessed on: 5 March 2022]
6. Miller AE, Olsson TP, Wolinsky JS, Comi G, Kappos L, Hu X et al. Long-term safety and efficacy of teriflunomide in patients with relapsing multiple sclerosis: Results from the TOWER extension study. Multiple Sclerosis and Related Disorders. 2020 Nov 1;46:102438.
7. Comi G, Freedman MS, Meca-Lallana JE, Vermersch P, Kim BJ, Parajeles A et al. Prior treatment status: impact on the efficacy and safety of teriflunomide in multiple sclerosis. BMC neurology. 2020 Dec;20(1):1-9.
8. Qiu W, Huang DH, Hou SF, Zhang MN, Jin T, Dong HQ et al. Efficacy and safety of teriflunomide in Chinese patients with relapsing forms of multiple sclerosis: a subgroup analysis of the phase 3 TOWER study. Chinese Medical Journal. 2018 Dec 5;131(23):2776-84.
9. Xu M, Lu X, Fang J, Zhu X, Wang J. The efficacy and safety of teriflunomide based therapy in patients with relapsing multiple sclerosis: A meta-analysis of randomized controlled trials. Journal of Clinical Neuroscience. 2016 Nov 1;33:28-31.










Comments (0)