Categories
Change Password!
Reset Password!


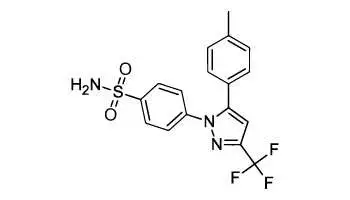
Celecoxib is a non-steroial anti inflammatory drug (NSAID) which is a selective inhibitor of cyclooxygenase-2 (COX-2). It works by reducing hormones that cause inflammation and pain in the body.
Celecoxib is a non-steroial antiinflammatory drug (NSAID) which is a selective inhibitor of cyclooxygenase-2 (COX-2). It works by reducing hormones that cause inflammation and pain in the body. Celecoxib is used in the treatment of rheumatoid arthritis and osteoarthritis. It is also used for ankylosing spondylitis.
Pharmacological Class: NSAID
Celecoxib, a selective COX-2 inhibitor, is classified as a NSAID, used to treat rheumatoid arthritis, osteoarthritis, and familial adenomatous polyposis (FAP). Celecoxib inhibits the prostaglandin synthesis. Unlike most NSAIDs, which inhibit both types of cyclooxygenases (COX-1 and COX-2), celecoxib is a selective noncompetitive inhibitor of COX-2 enzyme. It binds with its polar sulfonamide side chain to a hydrophilic side pocket region, close to the active COX-2 binding site. Both COX-1 and COX-2 catalyze the conversion of arachidonic acid to prostaglandin (PG) H2, the precursor of PGs and thromboxane.
Well absorbed in the gastrointestinal tract. When a single dose of 200 mg is given to healthy subjects, peak plasma levels occur 3 hours after an oral dose. The peak plasma level is 705 ng/mL. Absolute bioavailability studies have not been conducted. Volume of distribution is found to be 500 l/kg and plasma protein binding is 97%. Metabolism occurs in liver. Renal Excretion accounts for < 1% and plasma half life is ~97.
Common (affecting between 1 in 10 to 1 in 100)
Uncommon (affecting 1 in 100 to 1 in 1000)
Very rare (affecting less than 1 in 10,000)










Comments (0)