Categories
Change Password!
Reset Password!


High-intensity focused ultrasound ablation has proven to be a reliable long-term non-invasive therapy for uterine fibroids (or leiomyomas) with a high success rate and reduced need for re-interventions.
A recent study published in “BMC Women's Health” by Shuang Li and co-authors reported re-intervention of premenopausal women with uterine fibroids after ultrasound-guided high-intensity focused ultrasound (USgHIFU) ablation in the long-term and examined the aspects affecting re-intervention in case of non-perfusion volume ratio (NPVR) of ≥ 80% in patients.
Between 2012 and 2019, women with a single uterine fibroid who had undergone high-intensity focused ultrasound were registered. The subjects were stratified into 4 distinct groups as per the NPVR. Long-term re-intervention rates were examined using Kaplan-Meier survival curves, stratified by NPVR. In patients with an NPVR of 80% or higher, Cox regression analysis was employed to analyse the factors that influenced the likelihood of re-intervention.
Nine hundred twenty patients were successfully followed up out of 1,257 patients with uterine fibroids (median follow-up duration=88 months; median NPVR=85%).
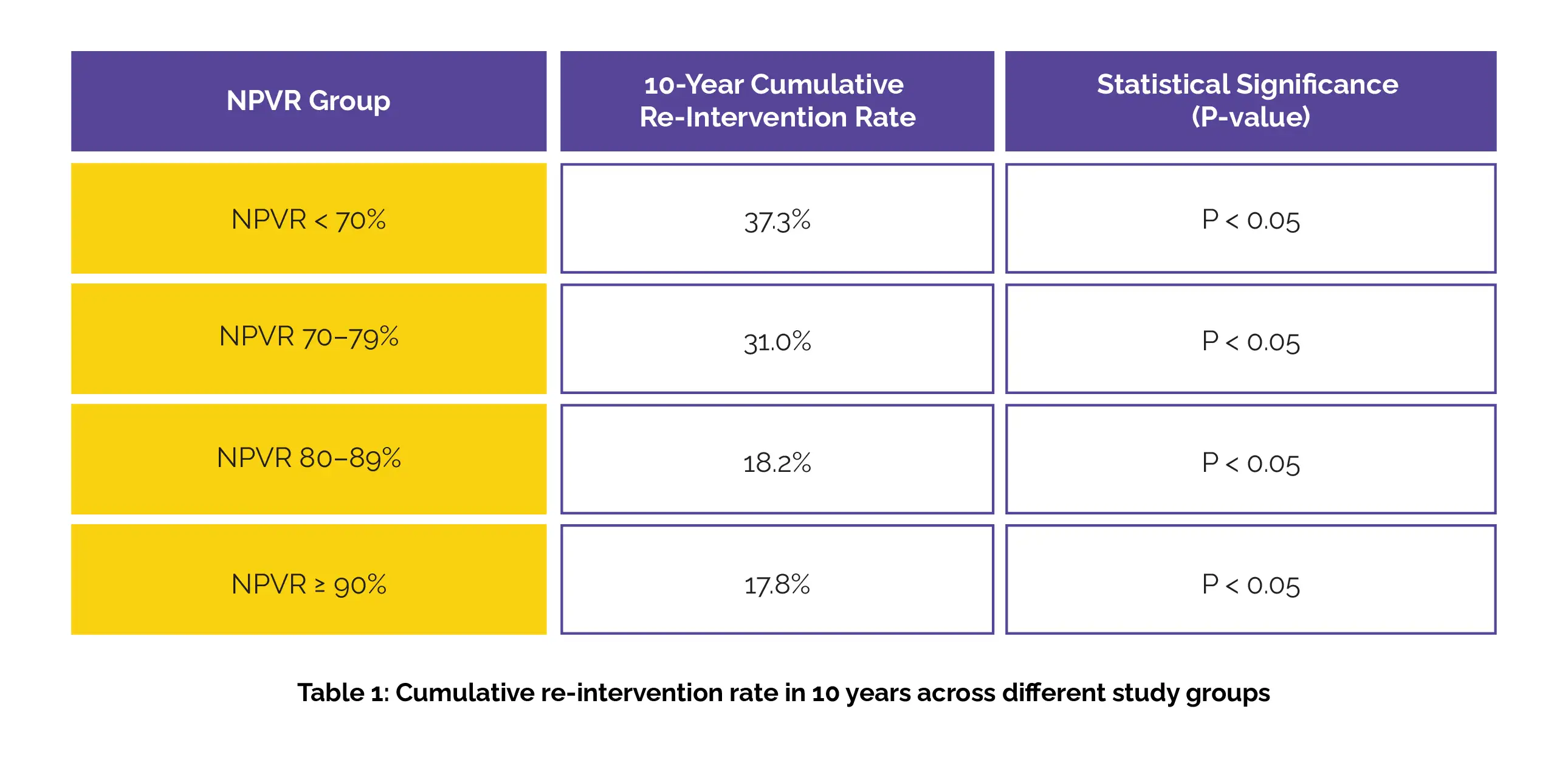
Cumulative re-intervention rates for USgHIFU-treated patients were observed as 3.4% at 1 year, 11.8% at 3 years, 16.8% at 5 years, 22.6% at 8 years, and 24.1% at 10 years. A notable difference was observed in the cumulative re-intervention rate at 10 years across the four NPVR groups, as mentioned in Table 1. Also, groups NPVR 80-89% and NPVR ≥90% (P = 0.499) showed no statistically significant difference.
In the NPVR ≥ 80% group, signal intensity on T2-weighted imaging of tumours and patient age were identified as independent predictors of long-term re-intervention. Younger patients and those with higher signal intensity on T2-weighted (T2W) images were found to be at higher risk of requiring re-intervention.
BMC Womens Health
Achieving NPVR ≥ 80% as technical success of high-intensity focused ultrasound ablation for uterine fibroids: a cohort study
Shuang Li et al.













Comments (0)