Categories
Change Password!
Reset Password!



Pain in the musculoskeletal system is common, especially when one performs tasks in awkward positions or engages in infrequent activities.
Turmeric-Boswellia formulation can effectively relieve exercise-induced acute musculoskeletal pain within 3 hours of administration.
Pain in the musculoskeletal system is common, especially when one performs tasks in awkward positions or engages in infrequent activities. Physical exercise has valuable effects. However, vigorous and eccentric exercises have a cost and injuries are quite common. Pain in the body's joints, muscles, ligaments, nerves, tendons, and systems that support the neck, limbs, and back might result from injuries or inflammatory disorders. The science of pain medicine has grown in recent years into a large speciality area. A major challenge for academics and clinicians continues to be the management of pain.
Oral analgesics are in high demand in both non-prescription and prescription drug markets. In a study, Ibuprofen and other over-the-counter analgesics did not result in an increase in the rate of skeletal muscle fractional synthesis after exercise. The typical rise in prostaglandin synthesis was inhibited. The isoform accountable for the COX-mediated rise in synthesis of protein was reported to be cyclooxygenase-1 (COX-1) enzyme. Further research is needed on the use of non-steroidal anti-inflammatory medicines to reduce moderate pain following acute or exercise-induced muscle damage. Considering alternatives for pain management has a lot of potentials.
Natural remedies are favored because they have a long history of usage in traditional medicine and are both safe and efficient in reducing inflammation and discomfort. Since ancient times, herbal remedies have been utilized to relieve pain effectively. Both turmeric and boswellia are well-researched anti-inflammatory substances that are becoming more and more popular. They are used as adjunctive as well as adjuvant to conventional therapy for musculoskeletal pain. Active components present in Boswellia serrata gum resin and turmeric rhizomes like boswellic acids and curcumin are known to suppress the nuclear-factor κB signaling pathway, which is connected directly to inflammatory processes.
Dietary supplements including Curcuma longa and B serrata are considered to be the most efficacious ingredients for osteoarthritis pain relief in the short-term. Since transient receptor potential channel, vanilloid subfamily member 1 (TRPV1) antagonists render the neurons implicated in pain inert, they are presently undergoing trials for indications linked with pain. Targeted neurotoxins that trigger neuronal death are another method of treating pain. TRPV1 is also activated by arachidonic acid derivatives that are found in the pain pathway. The pain-transmitting neurons become dormant as a result of all these activations.
Although herbal pain relievers are well-liked for controlling chronic pain, their use for acute pain has been constrained by their delayed onset of effect and shortage of rigorous clinical validation.
RATIONALE BEHIND RESEARCH
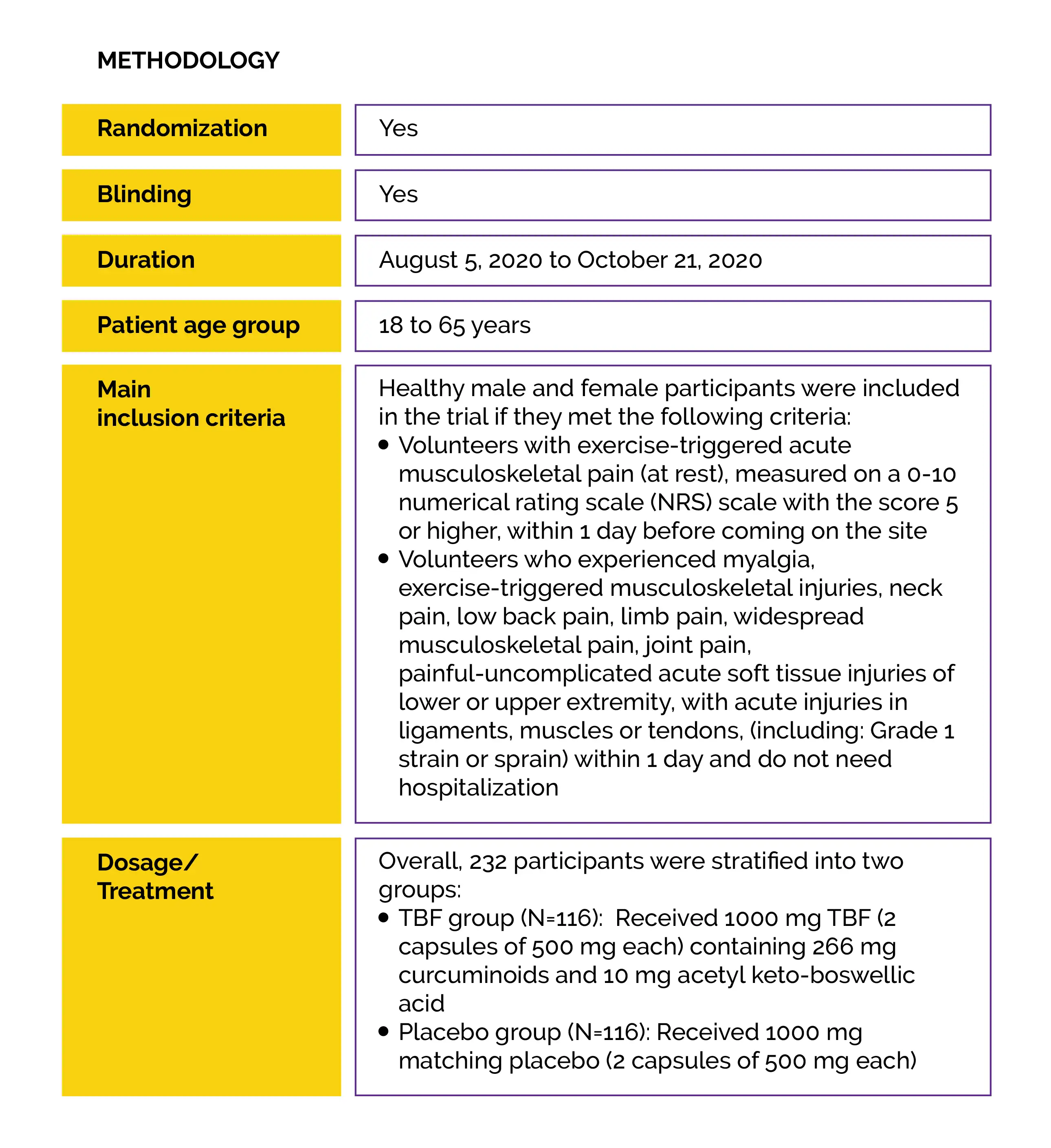
An active-controlled, open-label, single-center, pilot research was carried out for assessing acute musculoskeletal pain at the resting state, using turmeric and boswellia formulation (TBF) (1000 mg per day for 7 days). The results showed a similar pain-relieving effect to acetaminophen, most likely because of its ability to modulate multiple pain pathways quickly.
The current double-blind, placebo-controlled, multicenter study was designed to comprehend the impact of TBF on exercise-induced severe to moderate acute musculoskeletal pain and validate the results of the prior study using statistically significant sample sizes.
OBJECTIVE
The goal of this study was to assess the effectiveness of a single dose of 1000 mg TBF in minimizing exercise-triggered acute musculoskeletal pain, to examine the onset of pain relief and changes in pain intensity with movement and pressure applied to the injured area, with their effects on pain intensity at resting positions in healthy participants.
Study outcomes
Outcomes
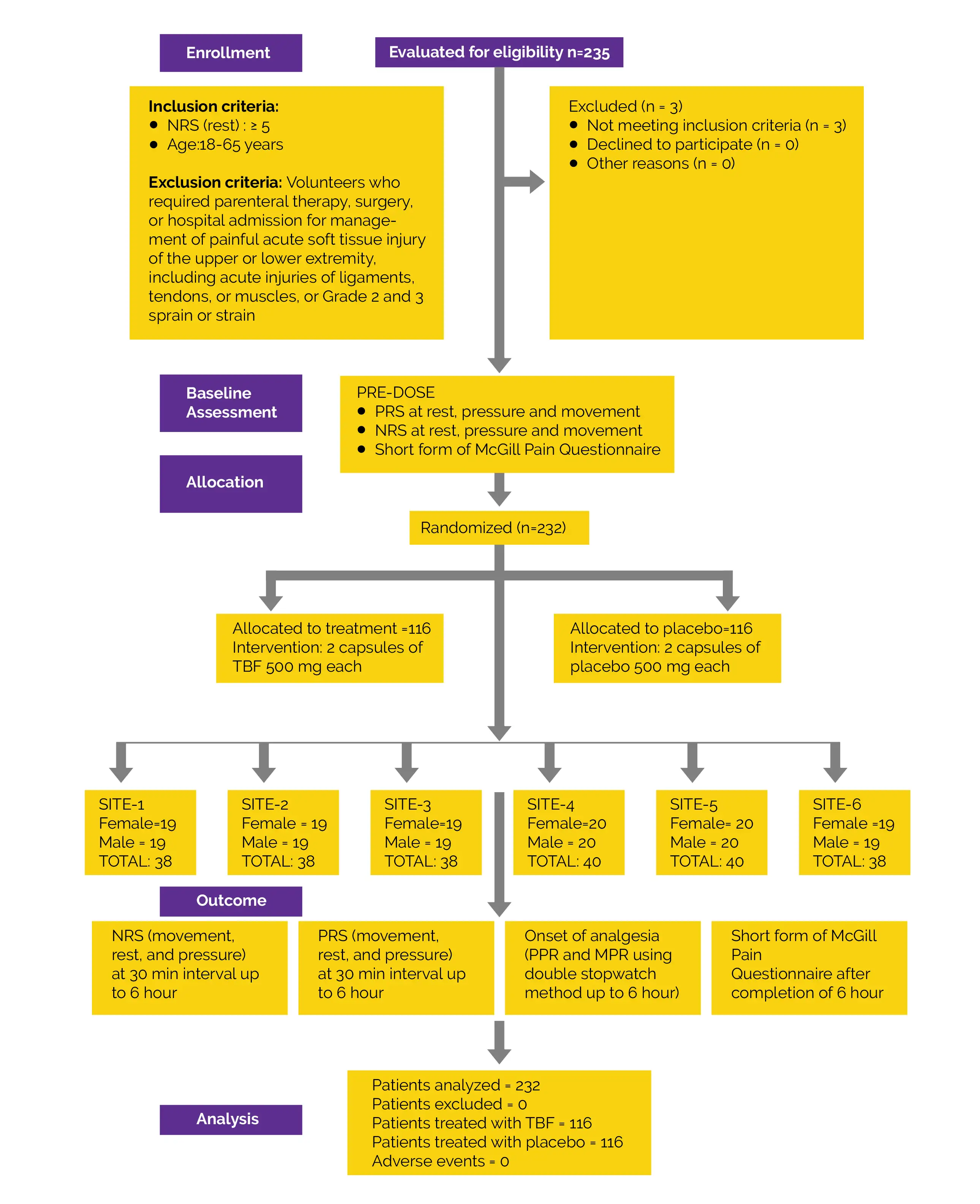
Baseline: There were no vital differences reported at baseline.
Study outcomes
In this research, the pain-relieving effect of turmeric and boswellia extracts formulation in sesame oil in minimizing exercise-elicited musculoskeletal pain was examined. TBF is a mixture of boswellia and turmeric. Prostaglandin E2 and cyclooxygenase 2 are both inhibited by curcumin in a time and concentration-dependent manner. In vivo studies demonstrated that curcumin exerts its analgesic effects by inhibiting the vanilloid 1, a transient receptor potential that is a critical component of nociception.
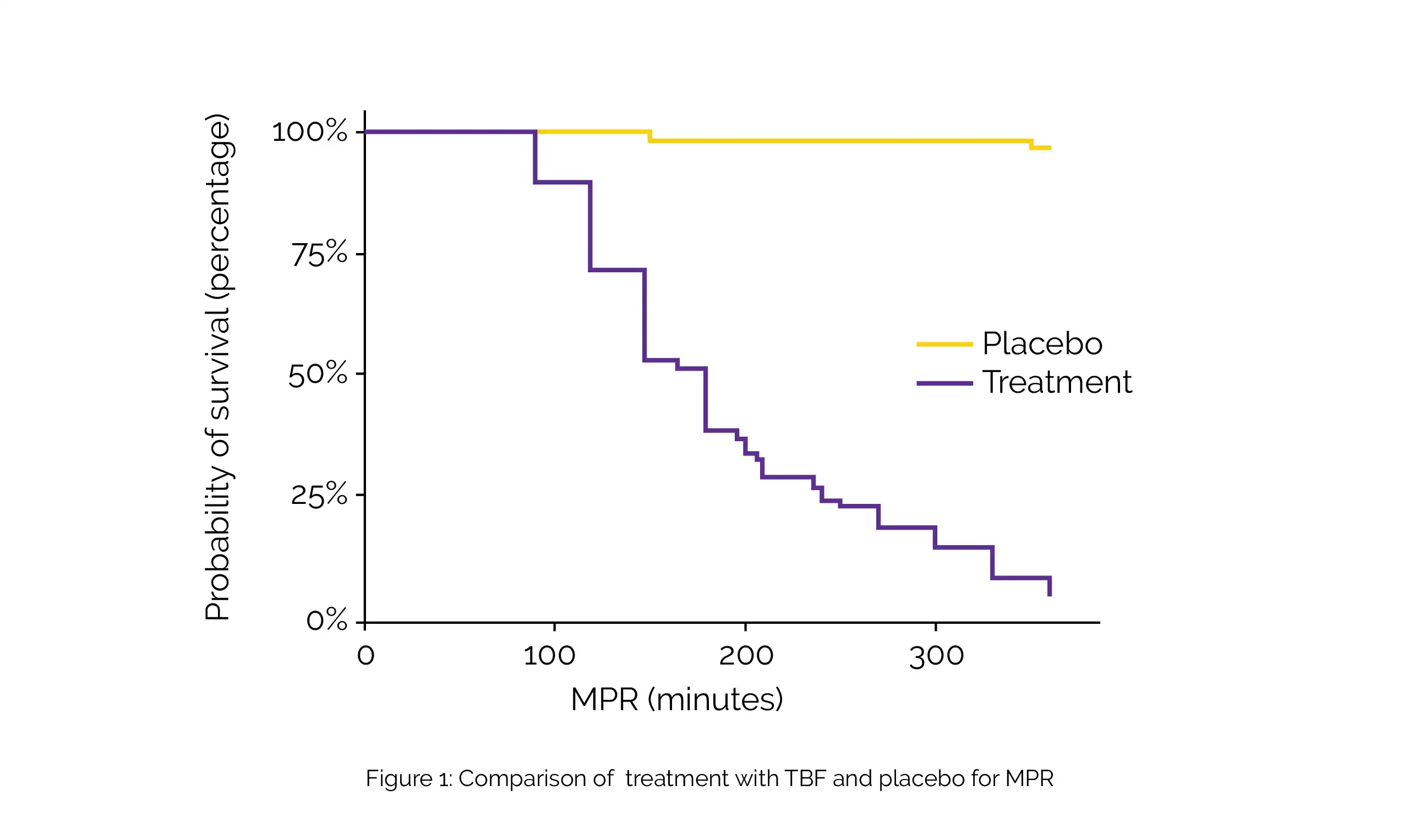
A systematic review and meta-analysis of eight trials revealed that curcuminoids substantially lessen pain. Boswellia and boswellic acids such as Acetyl-11-keto-β-boswellic acid (AKBA) have also been claimed to have analgesic properties. According to the current study, the presence of several naturally occurring anti-inflammatory agents in TBF may have contributed to the analgesic effect. These substances work to reduce acute and neuroinflammation as well as modulate various pain pathways. This may help to explain the quick onset of analgesia [MPR 191.6 minutes and PPR 68.5 minutes] with TBF as seen in the study.
Multiple interactions between pain and emotions affect how people perceive pain cognitively. Both the sensory and affective facets of pain responded favorably to TBF. Relative magnitudes of the sensory-intensive and emotional aspects of the various forms of pain before or after the therapy with TBF versus placebo show that TBF had a pivotal favorable impact on both the affective and sensory categories of pain. The placebo group's higher intraclass correlation coefficients (ICC) values for the MPQ total and the sensory domains compared to the affective category indicated a placebo effect, which is consistent with the results of prior investigations.
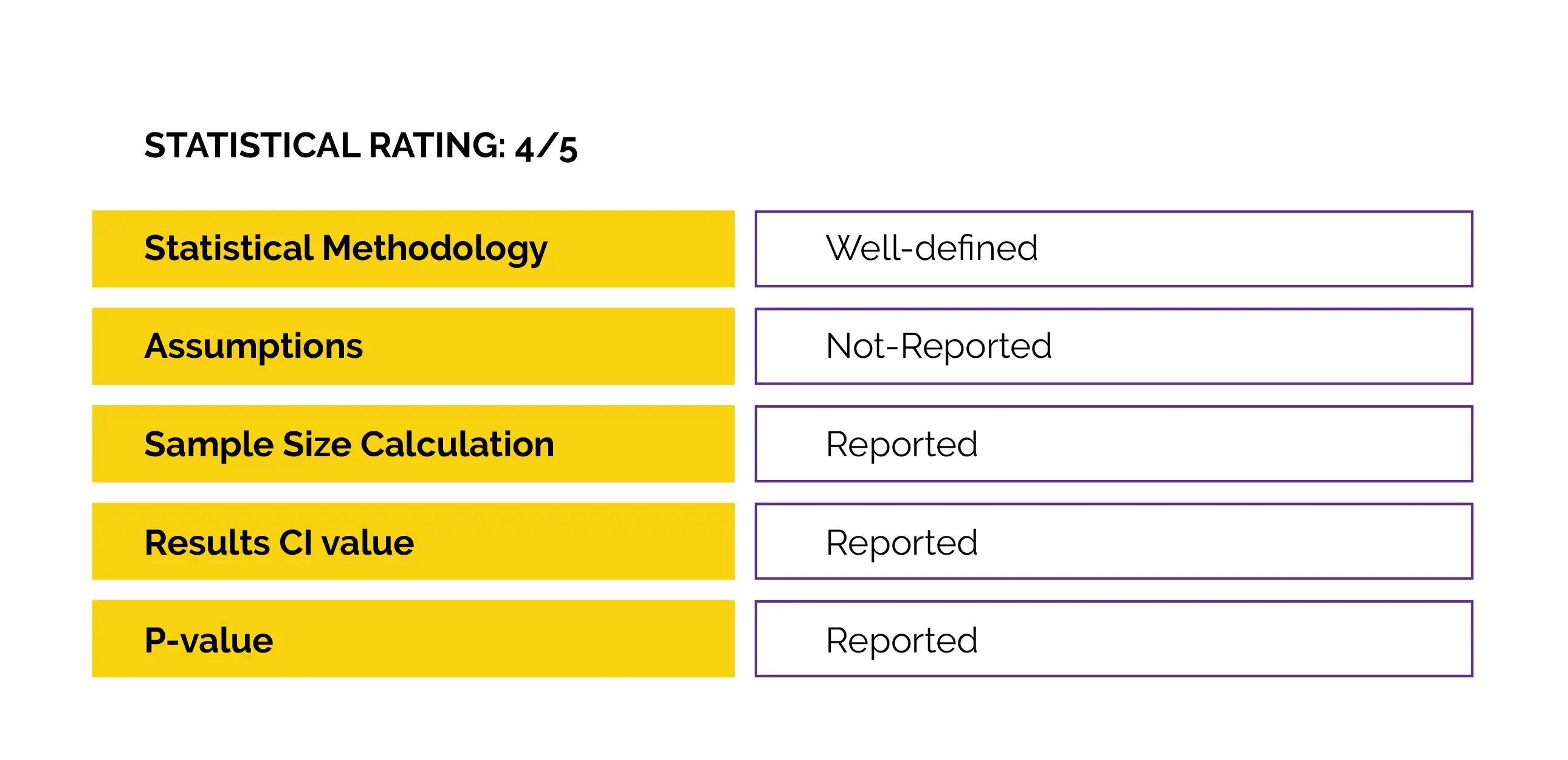
By examining treatment change beyond measurement error with the aid of SDD68, the common argument of measurement error with subjective pain questionnaires was overcome. For total, affective and sensory scales, the Sw values related to total score of respective scales were ≤10%. Thus, the measurement error in placebo arm was noted to be within acceptable bounds as determined by Ostelo et al. Due to considerable variation in the two assessments, the error of measurement in the TBF group was >20% demonstrating TBF efficacy in diminishing participants' pain.
With 93% of subjects having ≥50% of the maximal TOTPAR6, the repetitive proportional odds logistic regression revealed a continuous significant betterment in pain alleviation. The NNT is a useful indicator of how many individuals must get an analgesic intervention to experience at least 50% pain reduction over a 6-hour period. Of course, an NNT of 1 would be ideal, but in general, NNTs of 2 to 5 are suggestive of successful analgesic therapies. In the current investigation, for PRS (rest, movement, and pressure), the NNT was 1.1, indicating an excellent analgesic effect.
The likelihood of placebo effect cannot be ruled out due to placebo group's pain alleviation categorical scale results of 9.5% with pain symptoms improvement at rest, 7.8% on movement, and 6.9% on pressure. Previous research on acute pain and studies relating to exercise usually reveal a small placebo effect, frequently less than 5%. TBF and placebo both reduced pain in this trial, as shown by considerably negative time factors in repeated - measures proportional odds logistic regression. However, the odds of pain relief was lower in the case of placebo (0.00025 times that of the TBF).
TBF decreases musculoskeletal pain, as recorded by NRS, that demonstrated rapid analgesia commencement. It reduces the severity of pain and enhances psychological health as determined by the MPQ. A number of novel methods for treating pain revolve around processes that kill or exhaust the neurons responsible for transmitting pain. One strategy is to utilize targeted neurotoxins to trigger neuronal death while another strategy uses the transient-receptor potential vanilloid (TRPV1) for targeting neurons implicated in pain. Curcuminoids, primarily curcumin, are active ingredients found in turmeric roots. Although the precise mechanism of pain relief is uncertain, it is believed that curcumin can decrease pain that is TRPV1-mediated.
When TRPV1-binding agents aid calcium influx, the neuron loses its ability to operate. The calcium influx that results from prolonged or strong TRPV1 activation may cause the neurons to degenerate and die through a process known as apoptosis. With little impact on either cyclooxygenase (which makes prostaglandins) or 12-lipoxygenase, boswellic acids appeared to have a particular in vitro inhibitory function on 5-lipoxygenase. Increased concentrations of arachidonic acid, a substrate for COX-1, can decrease the effectiveness of AKBA's inhibitory action and make it reversible.
Boswellic acids can increase the release of arachidonic acid from human leukocytes and platelets, but they can also block the conversion of arachidonic acids to leukotrienes by 5-lipoxygenase. As a result, the mechanism of action differs significantly from that of traditional therapies, which block prostaglandin production.
This study relies solely on the subjective information provided by the participants; there are no biomarker analyses or positive controls in place.
Owing to its strong and potent analgesic activity, a single dose of 1000 mg of TBF can effectively treat exercise-triggered acute musculoskeletal pain of moderate to severe severity in around 3 hours. The onset of pain alleviation is prompt. Therefore, TBF can be recommended as a safe and efficacious natural remedy for acute pain management.
Medicine (Baltimore)
Fast pain relief in exercise-induced acute musculoskeletal pain by turmeric-boswellia formulation: A randomized placebo-controlled double-blinded multicentre study
Girish H Rudrappa et al.











Comments (0)