Categories
Change Password!
Reset Password!



When assessing the effectiveness of a 10 ml programmed intermittent epidural bolus (PIEB) in comparison to a 5 ml patient-controlled epidural analgesia (PCEA) without background infusion, it was discovered that the PIEB approach yielded several benefits.
The use of patient-controlled epidural analgesia is non-inferior to programmed intermittent epidural bolus when using equal volumes to maintain labor analgesia, and it outperforms the latter in terms of lowering local anesthetic consumption.
When assessing the effectiveness of a 10 ml programmed intermittent epidural bolus (PIEB) in comparison to a 5 ml patient-controlled epidural analgesia (PCEA) without background infusion, it was discovered that the PIEB approach yielded several benefits. These advantages included a reduced incidence of breakthrough pain, lower recorded pain scores, higher consumption of local anesthetics, and a similar level of motor block.
Consequently, a multicenter randomized controlled trial was conducted to investigate labor analgesia, involving the comparison of high-volume PCEA utilizing 10 ml boluses in each group against the PIEB technique.
The major endpoint of the study revolved around assessing two key factors: the occurrence of breakthrough pain and the total amount of analgesics consumed. Secondary endpoints under examination included motor block, pain ratings, patient contentment, and obstetric as well as neonatal results. The trial was deemed successful if it achieved two critical outcomes: (1) non-inferiority of PCEA with respect to breakthrough pain; and (2) superiority of PCEA with respect to local anesthetic use.
A total of 360 nulliparous females were randomized to either the PCEA-only group or the PIEB group. The PCEA group was given 10 ml boluses containing 0.12% Ropivacaine and 0.75 μg.ml-1 Sufentanil, while the PIEB group received 10 ml boluses along with an additional 5 ml PCEA boluses. Both groups had a 30-minute lockout period, and the maximum allowable hourly consumption of local anesthetic and opioids was the same for both groups.
The occurrence of breakthrough pain was comparable between the two groups, as depicted in Table 1:
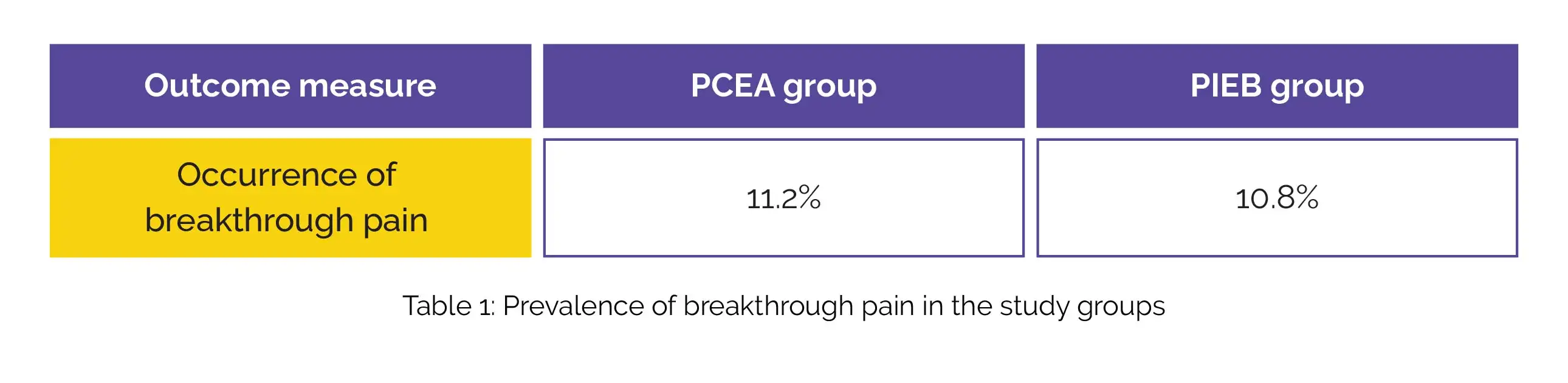
However, the total consumption of Ropivacaine was lower in the PCEA group, showing a mean difference of 15.3 mg. There were no significant differences in terms of motor block, patient satisfaction scores, or maternal and neonatal outcomes between the two groups.
When utilizing equivalent volumes of PCEA for maintaining labor analgesia, it is non-inferior to the PIEB approach. Additionally, PCEA demonstrates superiority in terms of local anesthetic consumption.
Anaesthesia
https://associationofanaesthetists-publications.onlinelibrary.wiley.com/doi/full/10.1111/anae.16060
High-volume patient-controlled epidural vs. programmed intermittent epidural bolus for labour analgesia: a randomised controlled study
E. Roofthooft et al.













Comments (0)