Categories
Change Password!
Reset Password!



Exercise-based cardiac rehabilitation (CR) improves health-related quality of life, reduces hospital admissions, and may lower mortality in heart failure patients, though most trials focused on heart failure with reduced (< 45%) ejection fraction (HFrEF) patients and were hospital-based, with limited diversity in representation.
Centre-based and home-based models, along with varying exercise types and intensities can be effective for personalized cardiac rehabilitation programs. Tailoring interventions to individual patient needs, such as considering the balance between aerobic and resistance training, could optimize outcomes in diverse patient populations with heart failure.
Exercise-based cardiac rehabilitation (CR) improves health-related quality of life, reduces hospital admissions, and may lower mortality in heart failure patients, though most trials focused on heart failure with reduced (< 45%) ejection fraction (HFrEF) patients and were hospital-based, with limited diversity in representation. This study aimed to evaluate the effect of physical therapy-based CR on fatality, hospital admissions and health-related well-being in those with HF.
The CENTRAL, MEDLINE, Embase, and three other databases were searched on 29 Jan 2018 and the bibliographies of systematic reviews and trial registers were also reviewed. Randomized trials comparing exercise-based CR interventions, with 6 months or more of follow-up against no exercise control (including usual medical care) in adults (≥18 years) with HF (HFrEF or HF with preserved (≥ 45%) ejection fraction [HFpEF]) were eligible. References were independently screened excluding ineligible studies, and full papers were retrieved for relevant trials. Data were extracted, risk of bias assessed, and GRADE analyses performed separately by the review authors.
Fourty-four trials with 5,783 HF participants and a median follow-up of six months, plus 11 new trials (1,040 participants) were included. Most studies focused on HFrEF patients in centre-based CR programs, but more studies included HFpEF patients and home-based CR. All trials had a no-exercise control, with various comparators like education or usual medical care. The overall risk of bias was low or unclear. CR exhibited little effect on short-term all-cause mortality (≤1 year) but reduced it in the long term (>12 months), Table 1:

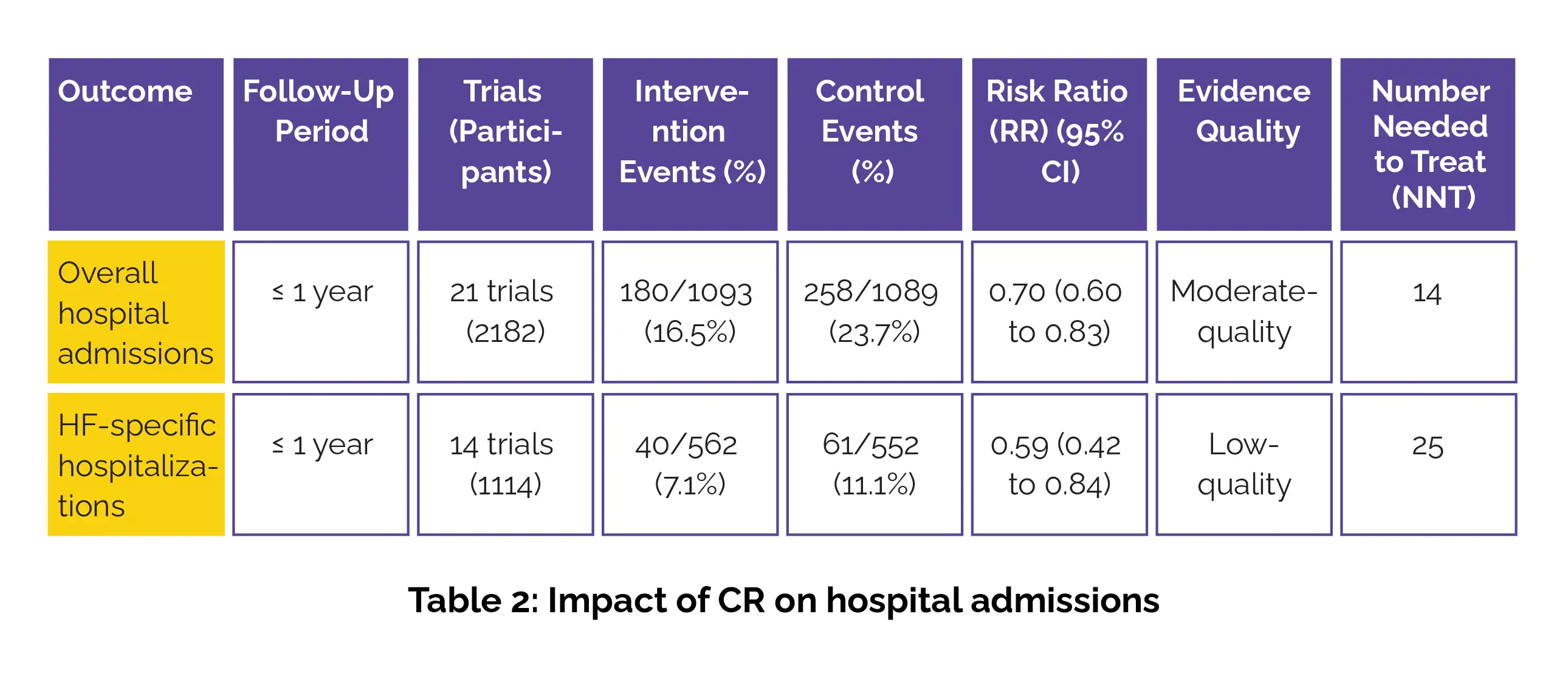
Regarding hospital admissions, CR probably reduced short-term hospital admissions and HF-specific hospitalizations, Table 2:
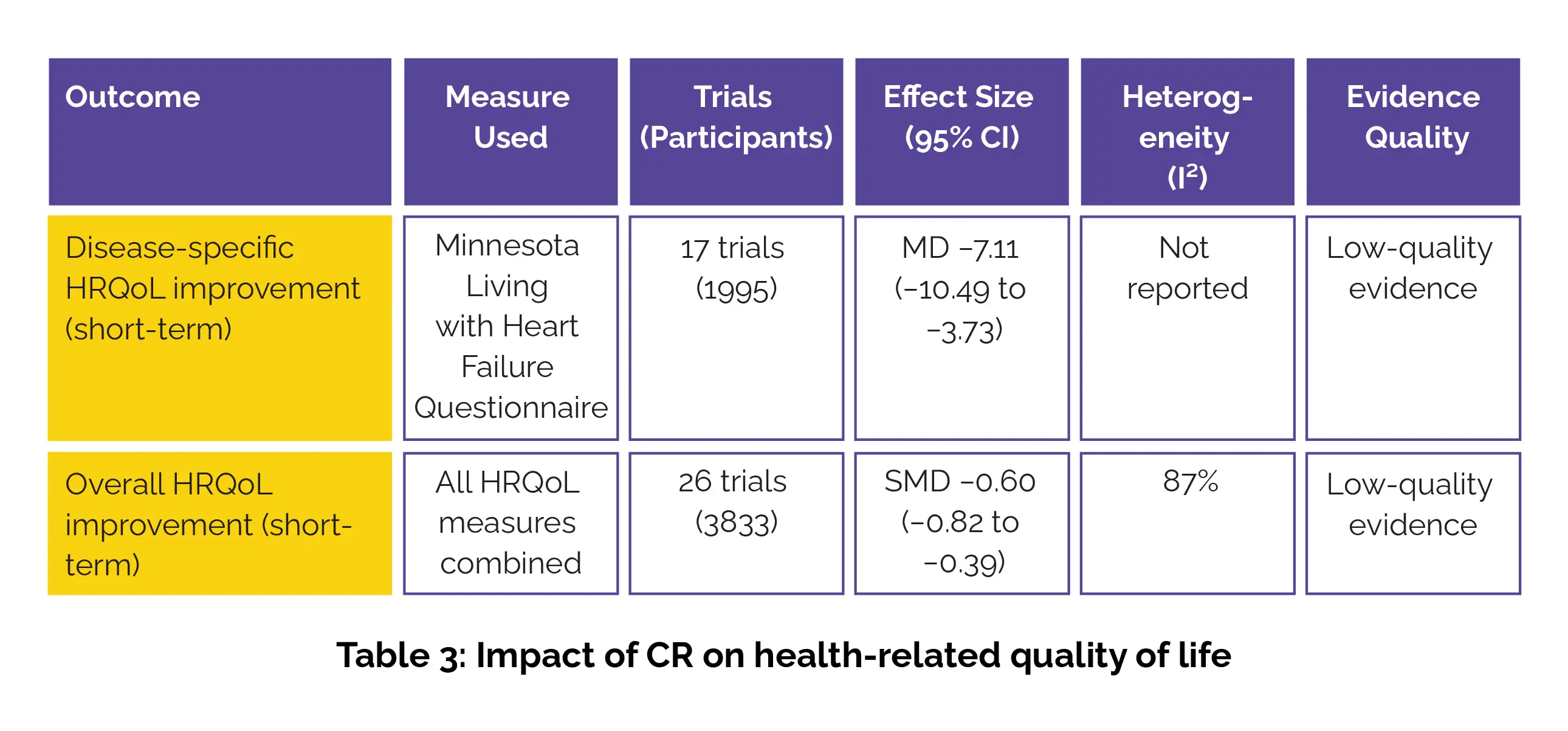
It improved short-term disease-specific quality of life, with a clinically significant improvement in health-related quality of life across all measures, Table 3:
The effects of exercise-based CR were consistent across different delivery models, exercise doses, and program types.
This updated review appends 11 trials to the 2014 Cochrane findings, displaying CR has no short-term (<12 months) impact on mortality. Moderate-quality evidence suggests CR likely reduces all-cause hospital admissions and may lower HF-specific admissions. While CR might improve health-related quality of life, the low evidence quality limits certainty. There is a need to consider underrepresented groups (older adults, women, HFpEF) and explore home- or technology-based CR programs in the future.
Cochrane Database of Systematic Reviews
Exercise‐based cardiac rehabilitation for adults with heart failure
Linda Long et al.













Comments (0)