Categories
Change Password!
Reset Password!



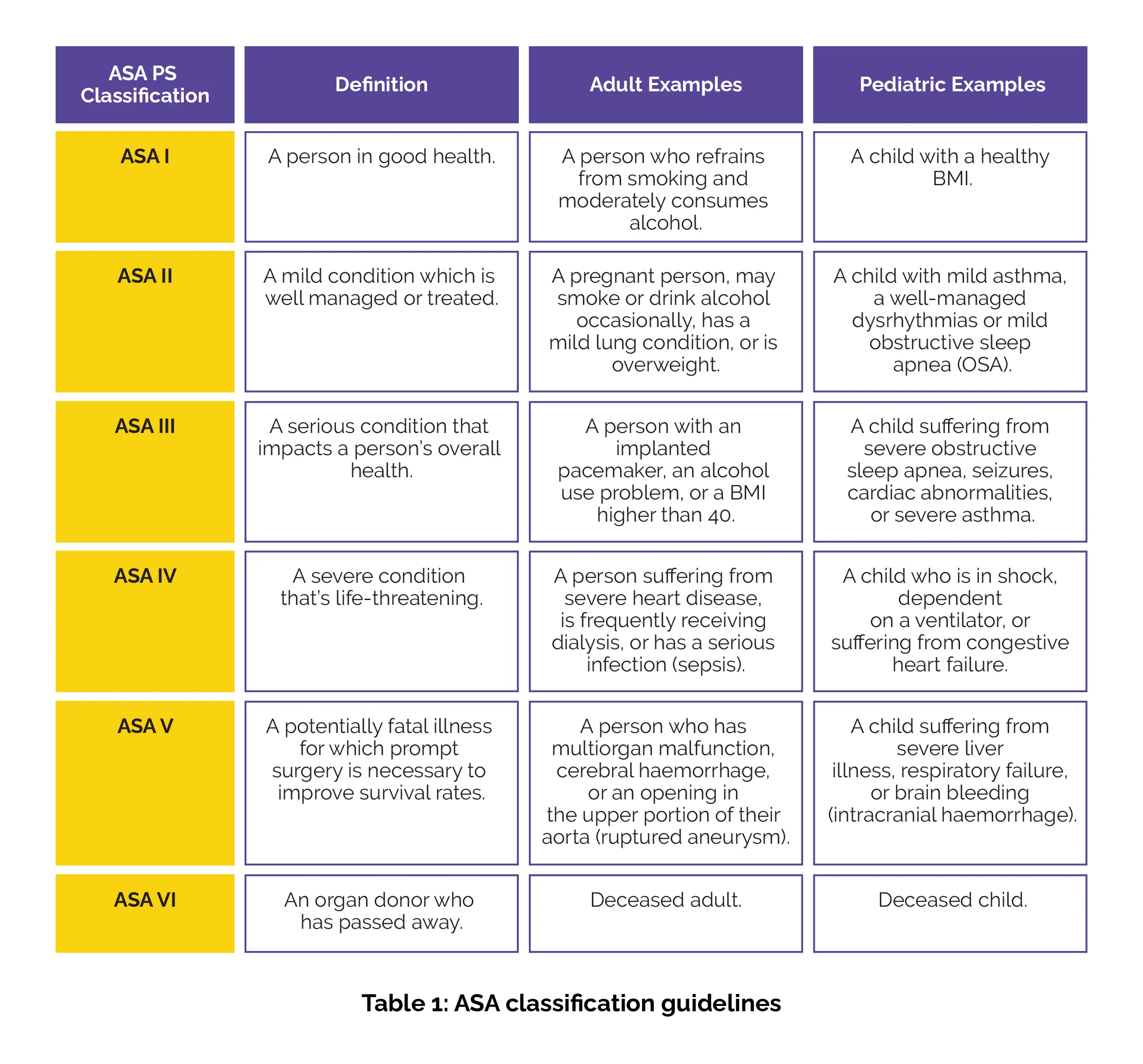
Postoperative pain accounts for the most prevalent complication in American Society of Anaesthesiologists (ASA) I, II and III groups of children. Over 80% of individuals experience acute postoperative pain.
The combination of Ibuprofen and Paracetamol, administered preoperatively and intravenously, has been shown to provide superior postoperative pain relief, enhance patient comfort, reduce the need for additional pain medications, and support quicker recovery in children.
Postoperative pain accounts for the most prevalent complication in American Society of Anaesthesiologists (ASA) I, II and III groups of children. Over 80% of individuals experience acute postoperative pain. It has been reported that maximum number of paediatric patients undergoing comprehensive dental treatment under general anaesthesia (GA) report discomfort from persistent bleeding and nausea, in addition to experiencing sore mouth, trouble eating, emotional distress, nightmares, mental discomfort, high anxiety, enuresis and altered behaviour. In order to reduce the financial burden, increase patient satisfaction, and avoid extended hospital stays, children receiving dental treatment under general anaesthesia (GA) must have their post-operative pain effectively managed. It is recommended by the American Society of Anaesthesiologists (ASA) that actions be taken "before, during, and after a procedure to reduce or eliminate postoperative pain before discharge." Additionally, research has demonstrated that factors such as the patient's age, anxiety level, kind of operation, and pre-existing preoperative pain all predict postoperative pain. Therefore, it is essential to assess various pharmacological interventions for effective post-operative pain relief.
RATIONALE BEHIND RESEARCH
Post-operative pain has been known to result in prolonged hospitalization and increased distress in 80-95% of the children receiving dental treatment under GA. Therefore, it is necessary to compare the multiple modalities used to control the post-operative pain in children so that the results presented can be employed by physicians to make an informed decision.
OBJECTIVE
The study aimed to explore the use of various pharmacological modalities to manage postoperative pain in children receiving general anaesthesia for dental treatment.
Literature search
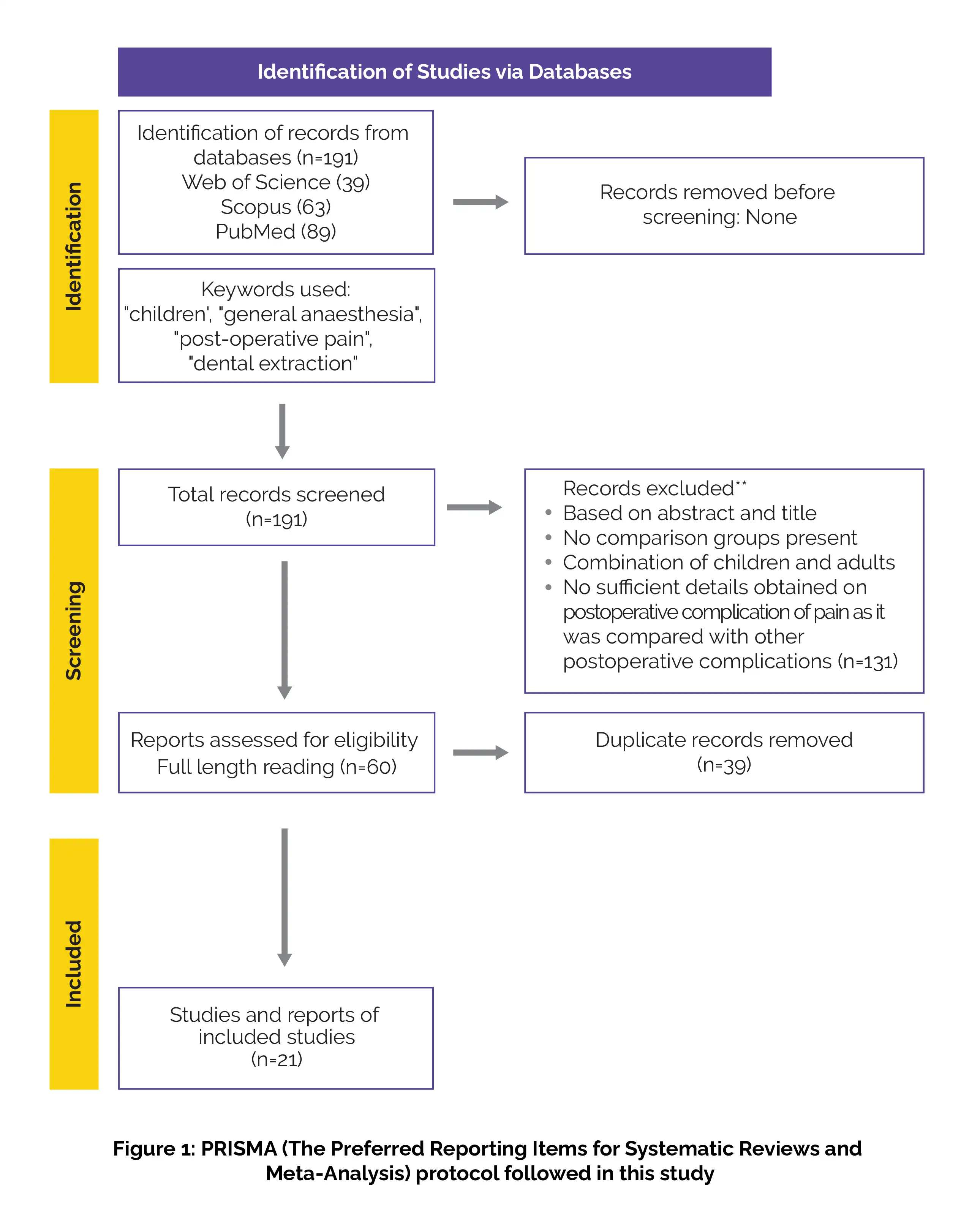
The systematic review adhered to the PRISMA criteria for systematic research and meta-analysis. Keywords like “children,” “general anaesthesia,” “postoperative pain,” and “dental extraction” were used in searches on Web of Science, Scopus, and PubMed for articles published up to June 2021. 131 abstracts were eliminated from the total of 191 abstracts based on the inclusion-exclusion criteria. Out of 60 shortlisted abstracts for full length reading and only 21 were selected for the systematic review after removing 39 duplicates.
Inclusion criteria
Exclusion criteria
Study Selection and Data extraction
The data was collected by two separate reviewers, and the third reviewer rectified any discrepancies. The data gathered included authors' names, publication year, country of origin, study type, demographic characteristics, treatment modalities, pharmacological agents used, frequency, procedure duration, postoperative pain intensity, analgesia, administration route, and outcomes.
The different pharmacological treatments to cure post-operative pain included the use of NSAIDs alone or in combination with opioid analgesics and local anaesthesia (LA). All the included studies utilized rescue analgesics by evaluating the pain score of the patient or as a routine regimen except for one RCT.
Data and Statistical Analysis
N/A
Risk of Bias and Quality assessment
The Joanna Briggs analysis was used to assess the risk of bias. The score of analysis >9 indicates low RoB, moderate if score is between 7-9 and high for score <7. The high RoB studies (2 studies) included the patients not randomized or systematically allotted into different analgesic groups. The post-operative pain assessment varied among the studies. The earliest assessments were made 15 minutes after recovery, while others observed pain levels for several hours post-anesthesia, with some extending follow-ups up to a week.
Outcomes
Study and participant characteristics:
Study quality:
Effect of intervention on the outcome:
Administration of NSAIDs alone or in combination with postoperative analgesia
Use of NSAIDs with opioid analgesics in postoperative analgesia
Use of opioids in postoperative pain management
Use of local anaesthesia alone or in combination with Paracetamol and NSAIDs in postoperative analgesia
Use of topical local anaesthesia alone in postoperative analgesia
Multiple studies suggest that preoperative administration of NSAIDs like Ibuprofen alone or in combination with Paracetamol effectively reduces postoperative pain scores due to the inhibition of prostaglandin release centrally and peripherally at the site of injury.
Children aged 2-7 years, experience higher pain scores and distress after teeth extractions compared to those aged 8-12. Two studies found that NSAIDs, such as rectal Voltarol and oral Diclofenac, significantly reduced postoperative pain scores compared to acetaminophen.
Another study involving a comparison among Ibuprofen, Ketoprofen, and Acetaminophen revealed that intravenous (IV) administration of Diclofenac improved postoperative analgesia, particularly in cases with multiple traumatic dental extractions. Diclofenac's action onsets in rectal administration at 20-24 minutes, avoiding first-pass metabolism, while oral Paracetamol has an onset of at least 1 hour and only 60% bioavailability after first-pass metabolism
Administration of Paracetamol preoperatively or IV Paracetamol intra-operatively instead of oral and rectal route has been shown to decrease the pain score rapidly. Preoperative oral Acetaminophen patients have been shown to require less rescue morphine postoperatively compared to rectal acetaminophen patients. Paracetamol's better preoperative analgesic effect is due to its serotonergic pain pathway mechanism, which interrupts the repeated firing of neurons from the surgical site.
A study reported that Rofecoxib administration required less postoperative analgesics than intra-operative administration, and rectal Diclofenac had peak analgesic effect at 30 minutes. However, a meta-analysis found no sufficient evidence to support preoperative analgesics for children under LA in dental clinics, as side effects include asthma, gastric bleeding, hepatotoxicity, and nephrotoxicity, warranting caution.
A short-acting opioid called Fentanyl when combined with NSAIDs was shown to decrease the pain score postoperatively in children. However, the use of IV Fentanyl is restricted in children receiving comprehensive dental treatment as it causes respiratory depression. In contrast, Sufentanil, an opioid agonist analgesic was found to be twice as potent as Fentanyl with no side effects. Another opioid agonist, Nalbuphine hydrochloride was shown to have superiority over morphine, however few side effects have been reported from its use as compared to NSAIDs.
Tramadol is a centrally acting opioid which functions by inhibiting the noradrenaline and serotonin (5HT) reuptake and providing analgesia from 20 minutes up to nine hours. However, its role in reducing postoperative pain is controversial due to no significant evidence and multiple side effects such as nausea, vomiting and respiratory reactions.
Intranasal analgesia is recommended using Dexmedetomidine and Midazolam due to rapid absorption and increased bioavailability compared to oral dosing. Dexmedetomidine is rapid, non-invasive, and has a has higher compliance rate but its use is limited by adverse effects like hypotension, bradycardia, and hemodynamic disturbances.
Long anaesthesia (LA), a pain reliever, may cause distress in young children due to its numbing effect. Intraligamental techniques are recommended for younger children to alleviate numbness and potential self-injury of lips, while morphine with or without IV NSAIDs is reported to cause less distress in postanaesthesia care unit nurses. The analgesic effect of LA only lasts for one hour, therefore rescue analgesics are needed to overcome postoperative pain. LA is essential for reducing haemorrhage in children, but it's inefficient for pain control. Furthermore, the topical use of bupivacaine did not alleviate postoperative discomfort.
FUTURE RECOMMENDATIONS
For children's postoperative discomfort, preoperative intravenous Ibuprofen and paracetamol are quite beneficial. Pain reduction may not be sufficiently achieved with local anaesthesia alone.
Journal of Clinical Pediatric Dentistry
Assessing modalities used to alleviate postoperative pain in children receiving dental treatment under general anaesthesia: a systematic review
Shivaranjhany Sivakumar et al.













Comments (0)