Categories
Change Password!
Reset Password!



To determine whether single or divided-dose Prednisolone causes more hypothalamic-pituitary-adrenal (HPA) axis suppression in first-time nephrotic syndrome treatment in kids.
For the first episode of pediatric nephrotic syndrome, single and divided-dose Prednisolone show similar efficacy for remission. But, single doses cause less hypothalamic-pituitary-adrenal suppression and delay relapse.
To determine whether single or divided-dose Prednisolone causes more hypothalamic-pituitary-adrenal (HPA) axis suppression in first-time nephrotic syndrome treatment in kids.
In an open-label randomized controlled trial, 60 children received Prednisolone (2 mg/kg/day) either as a single dose or in two divided doses for six weeks. This was followed by an alternative daily dose (1.5 mg/kg) for another six weeks. HPA axis suppression was assessed using the Short Synacthen Test and was defined as a post-adrenocorticotropic hormone cortisol level of less than 18 µ mg/dl.
While both dosing regimens effectively induced remission, divided-dose Prednisolone led to greater HPA suppression. However, children on divided doses experienced a shorter time to relapse (Table 1).
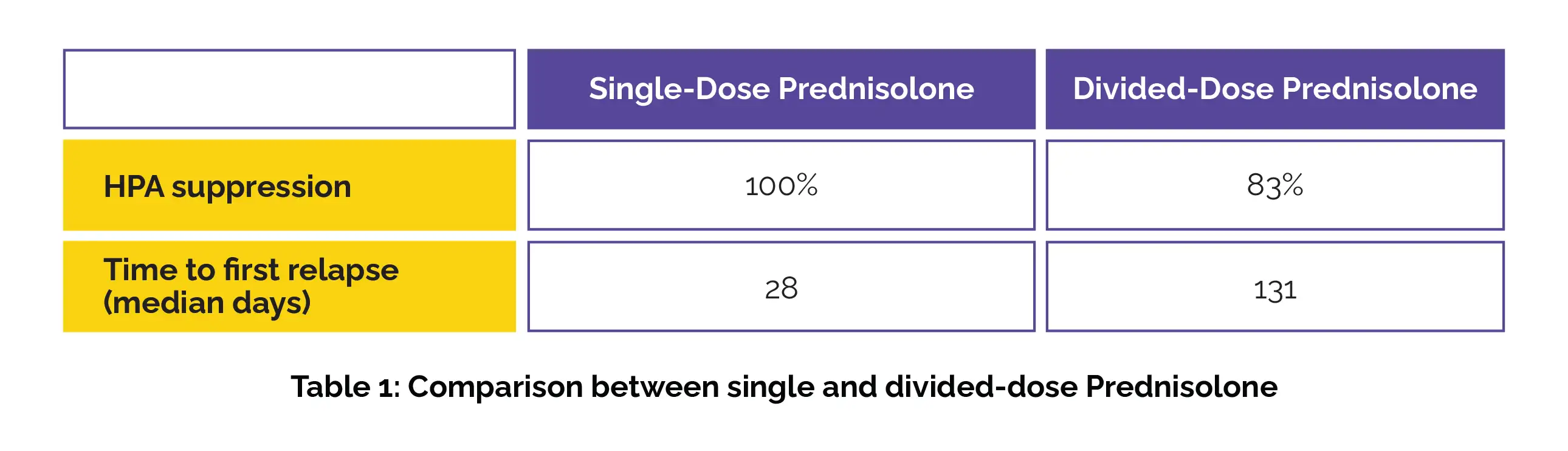
Single and divided-dose Prednisolone are equally useful for remission in nephrotic syndrome. However, single doses cause less HPA suppression, with a longer period before relapse than divided doses.
Clinical Journal of the American Society of Nephrology
Single- versus Divided-Dose Prednisolone for the First Episode of Nephrotic Syndrome in Children: An Open-Label RCT
Tania Khan et. al.













Comments (0)